OSCE on seizures
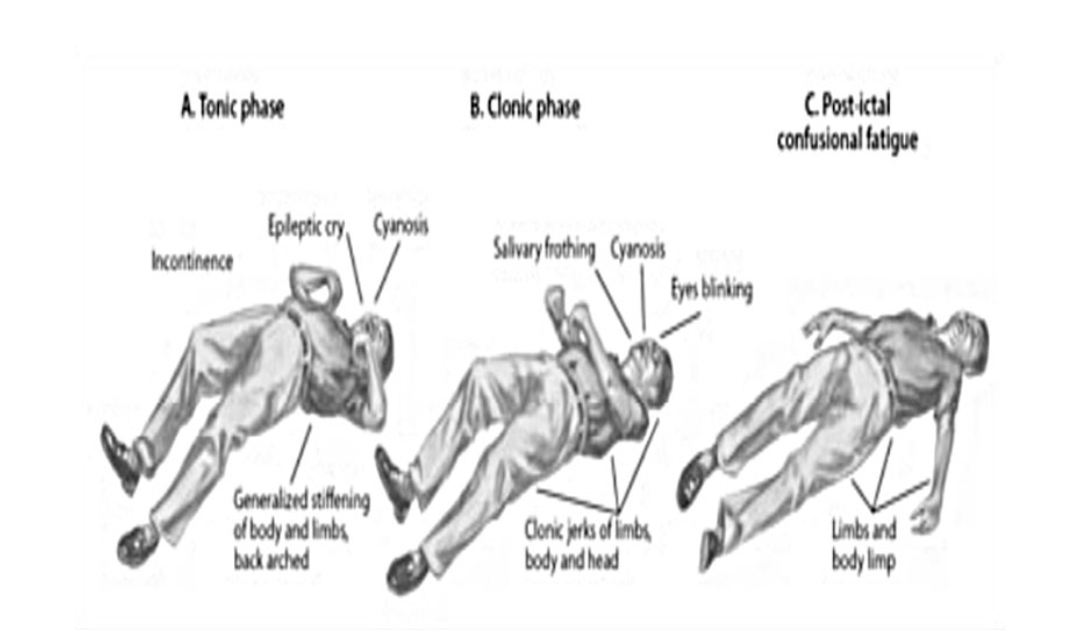
1. Differnce between seizures and epilepsy : Seizures are sudden, uncontrolled electrical disturbances in the brain that can lead to changes in behavior, consciousness, or movements. Epilepsy, on the other hand, is a neurological disorder characterized by recurrent and unprovoked seizures. In simpler terms, seizures are the individual events, while epilepsy refers to the condition of having multiple recurrent seizures over time 2.Status epileptic treatment Status epilepticus is a medical emergency characterized by prolonged, continuous seizures or multiple seizures without regaining consciousness in between. It requires immediate intervention. Treatment typically involves administering medications like benzodiazepines (such as diazepam or lorazepam) to stop the seizures, followed by antiepileptic drugs to prevent their recurrence. In severe cases, hospitalization and intensive care may be needed. If you suspect someone is experiencing status epilepticus, seek medical ...